Gastric or stomach cancer is relatively rare in the United States and other developed countries. Despite its rarity in the US, gastric cancer is the second leading cause of cancer-related death worldwide and is the fourth most common diagnosed cancer worldwide. The incidence rates for most types of gastric cancer are dropping worldwide due to improvements in living conditions and diet.1, 2
According to the American Cancer Society, it is estimated that in 2023, 26,500 cases of gastric cancer will be diagnosed and there will be 11,130 deaths from gastric cancer in.3
Below is a list of the information found within this section:
- Anatomy of the Stomach
- Types of Gastric Cancer
- Risk Factors
- Symptoms
- Detection and Diagnosis
- The Pathology Report and Staging
- Gastric Cancer Tumor Biology
- Treatment
- Resources
- Section Summary
Anatomy Of The Stomach
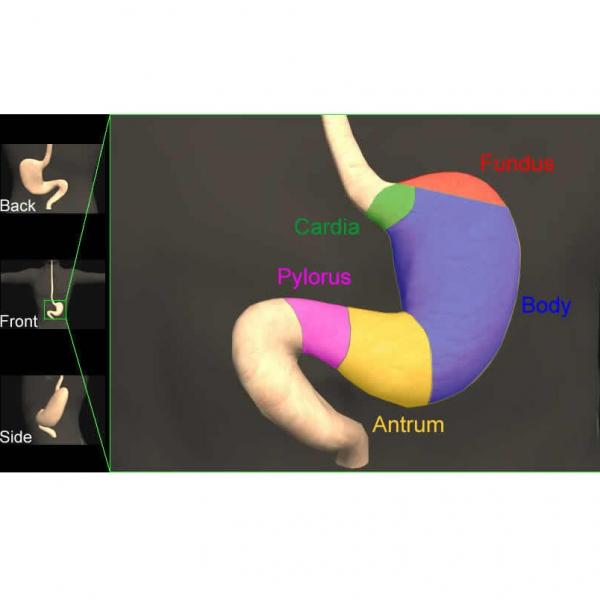
The stomach is a sac-like organ located between the esophagus and small intestine. The stomach aids in digestion and stores food. Anatomically, the stomach has been broken down into 5 different regions: cardia, fundus, body, antrum, and pylorus (see below). The stomach is also composed of 5 different tissue layers: mucosa, submucosa, muscularis, subserosa, and serosa. The more layers a cancer invades, the worse its prognosis.4
The stomach is also associated with an extensive lymphatic network. Cancer that has spread to the nearby lymphatics has a worse prognosis.5
Learn more about the lymphatic system.
Gastric Cancer: Types
Listed below are some common and uncommon types of gastric cancer:
Gastric adenocarcinoma - The most common gastric cancer. It is usually divided into two subtypes: intestinal and diffuse. Intestinal adenocarcinoma usually evolves in parts of the stomach closer to the intestines and more frequently affects people over the age of 80. Diffuse adenocarcinoma is found more often in young patients and those with blood type A. The diffuse form is what is traditionally considered gastric cancer.1, 6
Gastrointestinal Stromal Tumor (GIST) - Uncommon. Arises from cells in the Cajal that regulate intestinal contractions.7
Gastrointestinal Leiomyosarcoma - Uncommon. Rarely spreads to the lymph nodes. Arises from smooth muscle cells in muscularis mucosa or propria of the stomach lining.7
Gastrointestinal Carcinoid - Uncommon. Arises from the mucosa in the gastric body and fundus. Limited metastatic potential.8
Gastrointestinal lymphoma - Uncommon. Usually evolves in the stomach, but can start in any part of the gastrointestinal tract.9
Gastric Cancer: Risk Factors
Factors that influence the risk of developing stomach (gastric) cancer:
|
|
The relative effects of these and other risk factors in any given case of cancer is variable and very difficult to determine with accuracy at this time. Some of these and other risk factors are discussed below.
Helicobacter pylori infection
H. pylori is one of the most common bacterial infections worldwide. It causes duodenal and gastric ulcers as well as chronic gastritis. H. pylori significantly increases the risk of developing gastric adenocarcinoma. The World Health Organization classifies H. pylori as a class I carcinogen. It is found in the stomach of over half of the world's population. The bacteria live in the mucosal lining of the stomach and can cause chronic inflammation(gastritis). This inflammation can lead to DNA damage that promotes cancer development. H. pylori is associated with over 70% of gastric adenocarcinomas.
Eradication of the infection is the best way to prevent gastric cancer. A combination of antibiotics, stomach acid suppressors and stomach protectors may be used. Unfortunately, adequate diagnostic tests and drug therapy for H. pylori eradication is very expensive. A vaccine would be a better approach to the H. pylori problem. Vaccines have been moderately successful in animal models, but not in humans. Several types of vaccines are currently being studied.10
Diet
An increase in fiber, raw fruit, and vegetable consumption is associated with a significant decrease in gastric cancer risk. Consumption of nitrates, refined carbohydrates (white bread, white rice, sugary cereal, etc.) and highly salted or pickled foods is suspected to increase the risk for gastric cancer.10
Gender
Men are at higher risk than women for gastric cancer. This is especially true for the intestinal type of cancer. It is thought that female reproductive hormones such as estrogen and progesterone help protect against gastric cancer development.11, 12
Age
The risk for developing gastric cancer gradually increases after the age of 40. The diffuse type of gastric cancer occurs more often in younger patients whereas the intestinal type occurs more often in the elderly. For this reason, age is a greater risk factor for the intestinal type than for the diffuse type.11
Ethnicity and Geography
Caucasians are at the lowest risk of developing gastric cancer and people of Asian descent are at the highest risk. This disparity is mainly due to diet and living conditions. Japan and China have the highest rates of gastric cancer and H. pylori infection. Eastern Europe is also at a higher risk than North America and Western and Northern Europe.11, 1
Smoking
Studies have shown that smoking increases the risk for gastric cancer. Asian smokers have a higher risk for developing intestinal-type gastric cancer whereas Western smokers are at higher risk for diffuse type gastric cancer.11
Family History of Gastric Cancer
Cancer cases can be grouped into two broad categories, sporadic and familial. Sporadic cancers are those in which the affected individual does not have a known family history of the disease. Familial cancers tend to occur in several generations of a family and affected individuals often have close relatives (brother, sister, father) with the same type of cancer. It is possible that these individuals inherit genes that increase the risk for the development of specific cancers. Individuals with a family history of gastric cancer are at an increased risk of developing the disease. The increase in risk depends upon the type of relative affected. The more closely related an individual is to someone who has/had gastric cancer, the more likely they will share the associated genes. Inherited gastric cancer accounts for about 1-3% of all stomach cancer cases13.
The major gastric cancer susceptibility syndrome is called hereditary diffuse gastric cancer (HDGC). Other inherited forms of digestive system cancer include familial adenomatous polyposis (FAP) and hereditary non-polyposis colorectal cancer (HNPCC):
- Hereditary diffuse gastric cancer (HDGC): HDGC is an autosomal dominant disorder and is caused by a mutation in the CDH1 gene. The mutation results in a decrease in type 1 E-cadherin. This decreased expression appears to be the difference between diffuse and intestinal gastric cancer. The onset of cancer is widely variable for these individuals, from 16-82 years of age. Genetic testing is available for this syndrome.14Learn more about FAP and HNPCC.
Gastric Cancer: Symptoms
Symptoms
Early-stage gastric cancer typically has few symptoms, but the following general symptoms may occur:15
- Indigestion, stomach discomfort, or heartburn
- Nausea or loss of appetite
- Feeling tired
Late-stage gastric cancers are associated with the following symptoms:15
- Blood in the stool or stools that are black in color
- A bloated feeling after eating, even when eating a small amount
- Vomiting after meals
- Unintended weight loss
- Stomach pain, especially after meals
- Weakness and fatigue
Gastric Cancer: Detection And Diagnosis
Detection
In the US, gastric cancer detection occurs most often after it has developed into late-stage cancer. Because gastric cancer is not common in the US screening of the general public is not actively pursued. In contrast, countries that have high levels of gastric cancer, like Japan, have more rigorously applied screening procedures which often result in early detection of gastric cancer.16
Because about 1% of people infected wth H. pylori will develop gastric cancer, it has been proposed that screening for infection with the bacteria should be considered for people in the US living in areas where infection rates are high.17
For information about the methods used to detect cancer, refer to the Diagnosis and Detection section.
Gastric Cancer: The Pathology Report And Staging
The Pathology Report
If there is suspicion that a patient may have gastric cancer, a sample of tissue (biopsy) may be taken for examination. After a biopsy is taken, the physician who performed the biopsy sends the specimen to a pathologist. The pathologist examines the specimen at both the macroscopic (visible with the naked eye) and microscopic (requiring magnification) levels and then sends a pathology report to the physician. The report contains information about the tissue's appearance, cellular makeup, and state of disease or normalcy.
View more information about pathology reports.
Staging
Staging a cancer is a way of describing the extent of the disease. One of the most common methods used for cancer staging is called the T/N/M system. This system assigns a degree of severity based on the size, location, and spread of cancer in the body. Two important factors influencing survival for gastric cancer patients are depth of invasion through the gastric wall and the number of lymph nodes involved.15
Learn more about cancer staging and the TNM system.
Gastric Cancer: Tumor Biology And Genetics
Mutations (or epigenetic modifications) of key genes alter the behavior of cells. The genetic alterations lead to changes in protein products and changes in the amount of product produced by genes (gene expression). As changes accumulate, the cells become more abnormal and cancer progresses. Details about these changes can be found in the Mutation section. Some of the genes that have been shown to be important in the development of gastric cancer are listed and discussed below:
- CDH1 Gene
- TP53 Gene
- APC Gene
CDH1 Gene
CDH1 codes for a protein called epithelial cadherin or E-cadherin. This protein is involved in cell-cell adhesion and is responsible for the formation of organized tissues. E-cadherin also has roles in cell signaling, cell movement, and gene regulation. CDH1 functions as a tumor suppressor gene. Inherited CDH1 mutations are responsible for hereditary diffuse gastric cancer (HDGC) syndrome. Mutations in this gene also raise the risk for developing lobular breast carcinoma and prostate cancer.18, 19
TP53 Gene
TP53 is a tumor suppressor gene that encodes the protein product p53. It has been reported that TP53 is damaged (mutated) or lost in up to 80% of gastric cancers.18
Learn more about abnormal p53 and cancer development.
APC Gene
APC (adenomatous polyposis coli) is a tumor suppressor gene that plays a role in cell signaling. The APC gene is well known for its role in the development of colorectal cancer. However, mutations in this gene are also found in 60% of intestinal-type gastric cancers and 25% of gastric adenomas.18
Learn more about APC and cancer development.
Gastric Cancer: Treatment
Gastric cancer treatments can be divided into two categories based on the cancer: early stage and advanced stage. Early stage treatment involves tumors that have not yet penetrated the serosal layer of the stomach. Advanced stage treatment involves tumors that have penetrated the serosa and have spread to other regions of the body. Treatment options depend on the size and location of the tumor, the physical condition of the patient, and the cancer stage.
Surgery is the most common treatment option for early-stage gastric cancer. Three main surgical options exist for gastric cancer:
- Total gastrectomy - The surgical removal of the entire stomach
- Partial or subtotal gastrectomy - The surgical removal of specific sections of the stomach
- Resection - The surgical removal of a tumor and some surrounding tissue
The removal of the surrounding lymph nodes is frequently done during any type of surgery. Chemotherapy and radiation therapy may also be used after surgery. Gastric cancer has a high recurrence rate, so maintaining a healthy lifestyle and continuing medical surveillance after treatment are important.
Because our focus is on the biology of the cancers and their treatments, we do not give detailed treatment guidelines. Instead, we link to organizations in the U.S. that generate the treatment guidelines.
The National Comprehensive Cancer Network (NCCN) lists the following treatments for gastric cancer:
Information about clinical trials:
- General clinical trial information from CancerQuest
- Click here for information about clinical trials from the National Cancer Institute.
- Click here for information about clinical trials from Georgia Clinical Trials Online.
Gastric Cancer Resources
Risks for Gastric Cancer
Stomach Cancer Risk Factors (Moffitt Cancer Center)
Risk Factors: Stomach Cancer (CTCA)
Gastric Cancer Risks (MedLine)
Detection and Diagnosis of Gastric Cancer
Winship Cancer Institute: Make An Appointment
What You Need To Know About: Cancer of the Esophagus
What You Need To Know About: Stomach Cancer
Gastric Cancer Treatments
Gastric Cancer Treatment (NCI)
Treatment Choices by Type and Stage of Stomach Cancer (ACS)
Gastric Cancer Treatment (PubMed)
Gastric Cancer Survivorship
Living Beyond Stomach (Gastric) Cancer
Stomach Cancer Survivor's Guide
Long Term Risks for Gastric Cancer Survivors
Long Term Side-effects of Anticancer Treatments of Gastric Cancer
Side Effects from Radiation to the Stomach
International Gastric Cancer Resources
Cancer Research UK: Stomach Cancer
Stomach Cancer (Macmillan Cancer Support UK)
Cancer Council Australia: Stomach Cancer
Stomach Cancer (Australian Cancer Research Foundation)
Canadian Cancer Society: Stomach Cancer
Management of Gastric Cancer (Indian Council of Medical Research)
Section Summary: Gastric Cancer
Introduction
- Gastric cancer is the second leading cause of cancer-related death worldwide.
- Gastric cancer is rare in the US.
- Gastric adenocarcinoma is the most common type of gastric cancer.
Risk Factors
- Helicobacter pylori infection and diet are two of the most important risk factors.
- Men are at a greater risk than women.
- Inherited genes raise the risk for gastric cancer development. Hereditary diffuse gastric cancer (HDGC) syndrome involves inheriting specific forms of the CDH1 gene.
Symptoms
- Typically, early-stage gastric cancers are asymptomatic.
- Late-stage gastric cancers may cause abdominal pain, bloody stool or weight loss.
Pathology Report and Staging
- A biopsy of the tissue can be examined for tissue appearance, cellular makeup, and abnormalities.
- The T/N/M system is one of the most common methods used for gastric cancer staging.
- The T/N/M system assigns a degree of severity based on the size, location, and spread of the cancer.
Gastric Cancer Tumor Biology
- Many genetic changes occur in cancer. Details can be found in the Mutation section.
- One of the more common mutations in hereditary gastric cancer occurs in the CDH1 gene which acts as a tumor suppressor and plays a role in cell signaling.
Treatment
- Treatments may include surgery, radiation therapy, and chemotherapy.
- The lymph nodes surrounding the stomach are often removed during surgery.
- 1abc Hohenberger P, Gretschel S. "Gastric cancer." Lancet. 2003 Jul 26;362(9380):305-15. [PUBMED]
- 2 World Health Organization. "Global cancer rates could increase by 50% to 15 million by 2020." Switzerland. 3 April 2003. [http://www.who.int/mediacentre/news/releases/2003/pr27/en/]
- 3 American Cancer Society. (2023). American Cancer Society.Cancer Facts & Figures 2023. Atlanta: American Cancer Society. Retrieved from https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2023-cancer-facts-figures.html
- 4 Vander, Arthur J., James H. Sherman, Dorothy S. Luciano. Human Physiology, 6th Edition. McGraw-Hill, Inc. NY, NY (1994).
- 5 Detailed guide to stomach cancer. American Cancer Society (accessed August 2010). [http://www.cancer.org/Cancer/StomachCancer/DetailedGuide/index]
- 6 You WC, Ma JL, Liu W, Gail MH, Chang YS, Zhang L, Hu YR, Fraumeni JF Jr, Xu GW. "Blood type and family cancer history in relation to precancerous gastric lesions." Int J Epidemiol. 2000 Jun;29(3):405-7. [PUBMED]
- 7ab Katz SC, DeMatteo RP. "Gastrointestinal stromal tumors and leiomyosarcomas." J Surg Oncol. 2008 Mar 15;97(4):350-9. [PUBMED]
- 8 Levy AD, Sobin LH. "From the archives of the AFIP: Gastrointestinal carcinoids: imaging features with clinicopathologic comparison." Radiographics. 2007 Jan-Feb;27(1):237-57. [PUBMED]
- 9 Ghai S, Pattison J, Ghai S, O'Malley ME, Khalili K, Stephens M. "Primary gastrointestinal lymphoma: spectrum of imaging findings with pathologic correlation." Radiographics. 2007 Sep-Oct;27(5):1371-88. [PUBMED]
- 10ab Rocco A, Nardone G. "Diet, H pylori infection and gastric cancer: evidence and controversies." World J Gastroenterol. 2007 Jun 7;13(21):2901-12. [PUBMED]
- 11abcd Yoshida S, Kozu T, Gotoda T, Saito D. "Detection and treatment of early cancer in high-risk populations." Best Pract Res Clin Gastroenterol. 2006;20(4):745-65. [PUBMED]
- 12 Freedman ND, Chow WH, Gao YT, Shu XO, Ji BT, Yang G, Lubin JH, Li HL, Rothman N, Zheng W, Abnet CC. "Menstrual and reproductive factors and gastric cancer risk in a large prospective study of women." Gut. 2007 Dec;56(12):1671-7. [PUBMED]
- 13 Carneiro F, Oliveira C, Suriano G, Seruca R. "Molecular pathology of familial gastric cancer, with an emphasis on hereditary diffuse gastric cancer." J Clin Pathol. 2008 Jan;61(1):25-30. [PUBMED]
- 14 Lynch HT, Kaurah P, Wirtzfeld D, Rubinstein WS, Weissman S, Lynch JF, Grady W, Wiyrick S, Senz J, Huntsman DG. "Hereditary diffuse gastric cancer: diagnosis, genetic counseling, and prophylactic total gastrectomy."Cancer. 2008 Jun 15;112(12):2655-63. [PUBMED]
- 15abc Layke JC, Lopez PP. "Gastric cancer: diagnosis and treatment options." Am Fam Physician. 2004 Mar 1;69(5):1133-40. [PUBMED]
- 16 Graham DY, Asaka M. (2010) Eradication of gastric cancer and more efficient gastric cancer surveillance in Japan: two peas in a pod.J Gastroenterol. 45(1):1-8. Epub 2009 Aug 28. [PUBMED]
- 17 Tepes, B. (2009) Can gastric cancer be prevented?J Physiol Pharmacol. Dec;60 Suppl 7:71-7. [PUBMED]
- 18abc Zheng L, Wang L, Ajani J, Xie K. "Molecular basis of gastric cancer development and progression." Gastric Cancer. 2004;7(2):61-77. Review. [PUBMED]
- 19 Graziano F, Humar B, Guilford P. "The role of the E-cadherin gene (CDH1) in diffuse gastric cancer susceptibility: from the laboratory to clinical practice." Ann Oncol. 2003 Dec;14(12):1705-13. Review. [PUBMED]